

Patches of dirt in both city and rural settings can contain the spores of the fungus that causes Valley fever and are released whenever the ground is disturbed. (Photo by Jack Orleans/Cronkite News)
TUCSON – Daniel Sestiaga remembers being in the COVID-19 ward of a hospital in late 2020. He tested positive for the virus that causes COVID-19 in June, then later tested negative, but he was still struggling to breathe and testing positive again by the end of August.
After driving 60 miles to see his Indian Health Service primary care physician in Sells, Sestiaga said that his doctor took a chest X-ray showing pneumonia. His breathing became so difficult that he had to go to the emergency room before seeing a pulmonologist.
It wasn’t only COVID-19 causing his difficulty breathing. He was diagnosed with Valley fever after the X-ray revealed fluid around his lungs restricting their capacity. Sestiaga was told the fluid needed to be removed.
Doctors in the emergency room who were draining his lungs told him he was going to feel a lot of pressure and that he needed to keep breathing through the whole process. The capacity of his right lung was half its normal size.
Dr. Robert Johns is medical director of Banner Urgent Care. (Photo courtesy of Banner Health)
“All of a sudden, my lung started working,” Sestiaga said. “I could feel myself take a breath for the first time. After that they put me on a drain.”
The doctors wound up draining between 2 and 4 liters of fluid from his lungs, he said. He felt immense pressure.
Valley fever (Coccidioidomycosis) is an infection caused by the spores of Coccidioides fungus, according to the Centers for Disease Control and Prevention. The spores live in the soil and dust in some areas of the southwestern U.S. People become infected by inhaling the spores when they’re released from the dust.
When they tested Sestiaga, they noted that his markers for infection with Coccidioides were “through the roof,” he said.
Testing early may prevent a lot of the problems associated with the progression of the disease, according to Dr. Robert Johns, medical director of Banner Urgent Care. Johns recalled one person experiencing serious complications after not being tested quickly enough.
“This individual who’d been diagnosed with pneumonia at the ER, given an antibiotic, actually had Valley fever,” Johns said. “He was admitted to the hospital in the ICU. He was put on a ventilator and ended up having a pneumonectomy, that’s part of the lung removed.”
Dr. John Galgiani, director of the Valley Fever Center for Excellence at the University of Arizona. (Photo courtesy of Kris Hanning, Biocommunications, University of Arizona Health Sciences)
Because of greater awareness of the disease, anyone who comes to Banner Urgent Care with pneumonia should receive a Valley fever test, Johns said. Sometimes, the disease also produces a telltale rash called erythema nodosum that may warrant a prompt test.
“One, it’s not going to clear up with antibiotics. Two, it’s more than likely going to get worse,” Johns said.
Despite that, tests aren’t typically sensitive in the early course of the disease, said Dr. John Galgiani, director of the Valley Fever Center for Excellence at the University of Arizona.
“It’s a very specific test. If it comes back positive, even a single test, you don’t need to wait for a pair,” Galgiani said. “Unfortunately, they’re not completely sensitive so that early in the course of these tests, sometimes they’re negative. When you repeat it two weeks later, it turns positive.”
The tests also often need to be sent to an outside laboratory – in-clinic tests aren’t yet commonplace – which can lead to delays that impede treatment, Galgiani said.
“That delay is actually an impediment to the test getting done at all because it seems like it’s going to come back long, too long to be really a problem,” Galgiani said.
According to the CDC, the true number of Valley fever cases is likely underreported due to many patients not being tested. The Valley Fever Center for Excellence estimates that the actual number of cases is six to 14 times higher than reported.
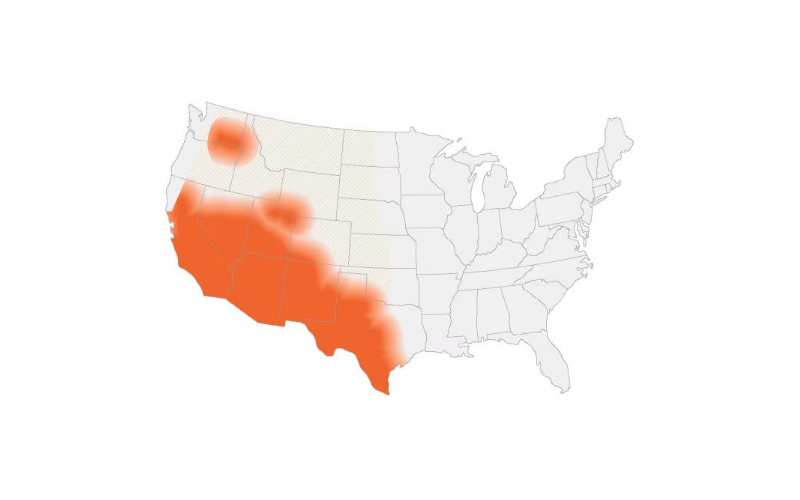
Estimated areas with coccidioidomycosis (Valley fever) in the United States. (Map courtesy of CDC)
The fungus is found throughout the Southwest and, according to the Arizona Department of Health Services, Arizona accounts for nearly two-thirds of all Valley fever cases in the U.S.
Between 1990 and 2022, reported cases of Valley fever climbed from 5.2 per 100,000 people, to 128.4 per 100,000 people, according to the Arizona Department of Health Services. Arizona’s top three most populous counties alone – Pima, Maricopa and Pinal – made up 94.1% of Valley fever cases in the state.
In addition, Valley fever is one of Arizona’s most commonly reported infectious diseases. In 2022, there were 706 hospitalizations associated with a primary diagnosis of Valley fever, and hospital charges for Valley fever patients totaled $68.3 million, according to the Arizona Department of Health Services.
“It’s kind of an Arizona disease now because of population growth in the state. Whereas originally the name came from California,” Galgiani said. “Between those states 95% of infections occur.”
Although Arizona has the highest rates of patients with the disease, the fungus that causes Valley fever can be found throughout the Americas, from Mexico to Argentina, Galgiani said.
Most people recover from the disease without medical care, and approximately 60% of people experience no symptoms. But in some cases the infection travels throughout the body, known as dissemination, according to an article in the Journal of Fungi. Out of 150,000 estimated infections in the U.S, approximately a third require clinical attention.
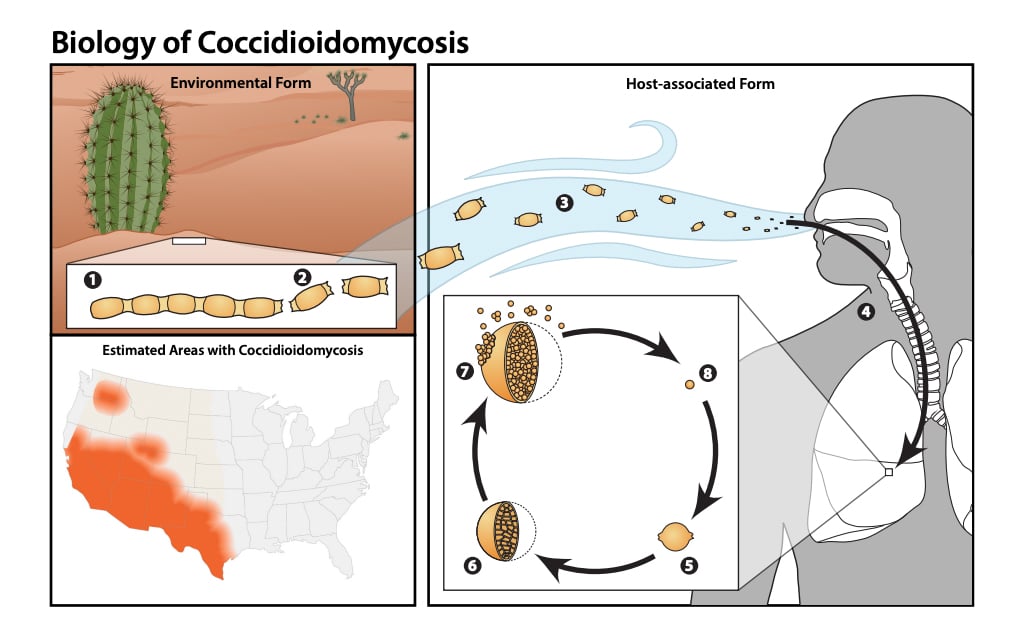
Biology of Coccidioidomycosis. (Graphic courtesy of CDC)
The main symptoms of acute infection include fever, cough, shortness of breath and rash, according to several health sources. Symptoms of chronic infection include coughing blood, low-grade fever, weight loss, chest pain and nodules in the lungs.
In severe cases of dissemination, the fungus may cause severe nodules or lesions worse than those initially present; painful lesions in the skull; painful, swollen joints; and meningitis, according to several health sources.
Anyone can contract the disease but infection varies between races and ethnicities. In Arizona, Hispanic, Native American and Black people are more likely to have severe Valley fever than white people.
A study reported in a 2019 article in the Open Forum Infectious Diseases journal, looked at the disease in American Indians/Native Alaskans from 2001 to 2014, and found they had high hospitalization rates, high morbidity and possible missed opportunities for earlier diagnosis. The study concluded that Native Americans “may be uniquely vulnerable” to Valley fever.
Sestiaga is a member of the Fort Yuma Quechan Tribe.
“A lot of Native people had let me know, ‘Well, I had a cousin who died, and I had this uncle who passed away,’ and then they found out later on it was Valley Fever,” Sestiaga said.
Before being diagnosed with the disease, Sestiaga said he didn’t even know about Valley fever. Despite the advances in testing, there’s still a lack of awareness about testing for it in pneumonia cases, Johns said. There’s also a lack of knowledge for doctors trained where the disease isn’t endemic, especially on the East Coast.

Daniel Sestiaga experienced a severe case of Valley fever and went to the emergency room for it twice. (Photo by Jack Orleans/Cronkite News)
“I had to do a crash course on Valley fever. ‘What is it?’ What’s going on?’ I had recently gotten my masters of public health from U of A, but Valley Fever never came up in the conversation. I never even knew what Valley fever was,” Sestiaga said.
Valley fever is treated with azole antifungal drugs, like fluconazole. If treatment is stopped, a relapse in infection can occur, according to the Journal of Fungi. Galgiani said there’s no vaccine yet, however, there’s a push to start human trials as early as this year.
“I’ll probably be on a low-dose (of) fluconazole for the rest of my life,” Sestiaga said.
Some of the side effects of fluconazole include peeling or loosening of the skin, hair loss, chest pain, muscle pain and spasms and unusual bleeding or bruising, among others, according to several health care providers.
“I couldn’t even complete one round because they had to put in the IV. They had to fill you with a whole bag of saline (and) fluid because it’s just so hard on your kidneys,” Sestiaga said. He was given a cocktail of drugs in the hospital, including fluconazole and amphotericin, he said.
Galgiani said part of the reason that funding has been slow to find a vaccine is because Valley fever is an “orphan disease,” defined by the Food and Drug Administration as a disease that affects fewer than 200,000 people. So far, the only tools to combat Valley fever are education on how to prevent the disease and antifungal treatments.
Research may also suffer from a lack of willing participants. Sestiaga only signed up for medical studies that focused on Valley fever and nothing else. His caution came from knowing the history of mistreatment of Indigenous people in medical settings.
Related story

In 2004, the Havasupai tribe sued the Arizona Board of Regents and Arizona State University when tribal members discovered that DNA samples taken for research on type 2 diabetes had been used in other genetic studies as well, without their consent.
According to the American Medical Association Journal of Ethics, researchers violated the tribe’s informed consent by testing their genetic material for inbreeding, schizophrenia, alcoholism and the origin of the tribe’s migration from Asia.
“Culturally, I’m really not supposed to be giving you my blood, (that’s) just what we were taught,” Sestiaga said.
It’s also difficult to measure Valley fever infections in those who work outdoors. Any activity that involves digging, soil disruption or generating dust in places where the Coccidioides fungus grows puts workers at risk for infection, according to the Occupational Safety and Health Administration.
Valley fever isn’t covered under Arizona worker’s compensation, according to the Industrial Commission in Tucson. Over one-third of construction workers in Arizona lack health insurance, almost three times the rate for all workers, according to the Labor Center at the University of California in Berkeley.
Even with insurance, proper treatment isn’t a guarantee.
“I had the ability to have the coverage … to be able to cover, obviously, the treatment, everything,” Sesitaga said. “But it doesn’t come without its hiccups.”